Saint-Étienne, France

Dr. Marie-Caroline Trone
Hospital-based Ophthalmologist at Saint-Étienne University Hospital – France
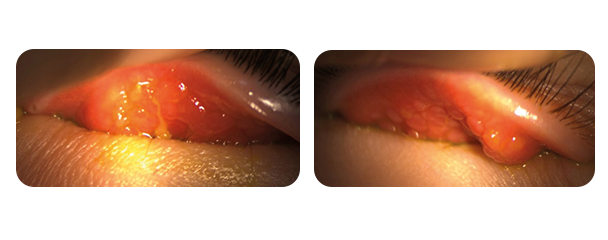
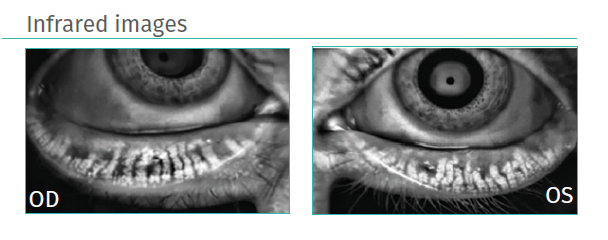
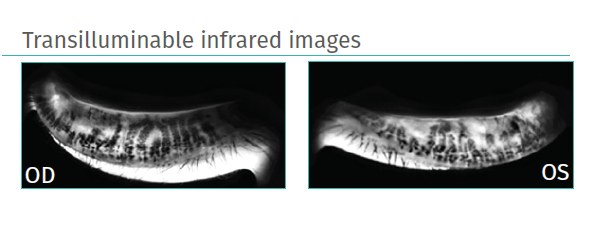
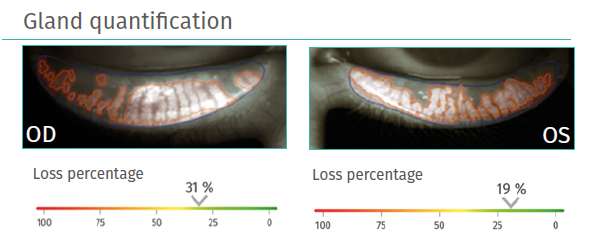
Diagnosis and treatment of a child with vernal keratoconjunctivitis (VKC) associated with meibomian gland dysfunction (MGD). A full diagnosis was made via clinical examination and meibography using C.Diag®. Intense Pulsed Light treatment using the C.Stim® IPL system was started for the patient. After 6 months, meibum quality had improved with an expressible, fluid consistency.
Anamnesis :
Paul, an 8-year-old schoolboy, sought urgent medical attention after experiencing red, painful eyes for several days (in April). He was highly sensitive to light. He was in good health and not taking any medication but has seasonal pollen allergies.