Saint-Étienne, France

Dr Marie-Caroline Trone
Hospital-based Ophthalmologist Saint-Étienne University Hospital – France
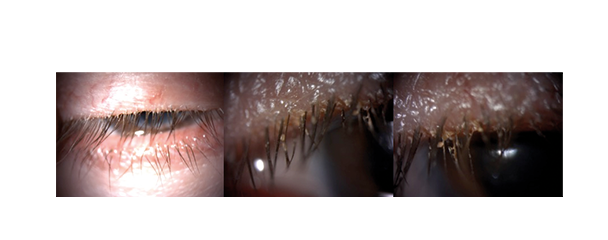
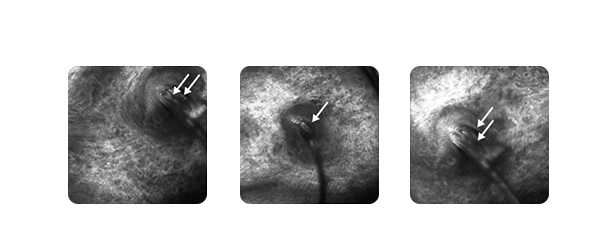
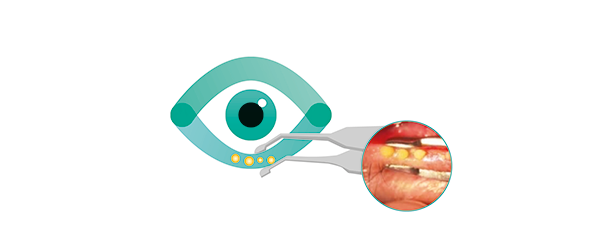
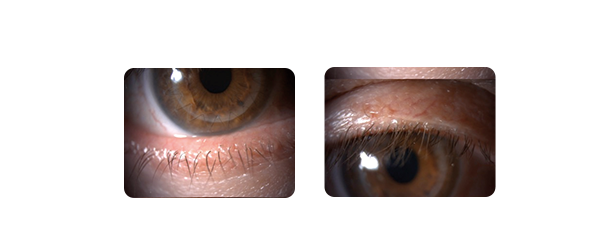
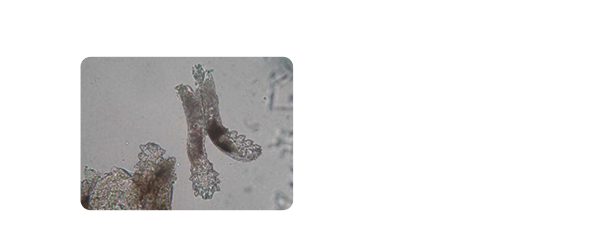
Diagnosis and treatment of dry eye syndrome (DES) in a male patient with Demodex blepharitis leading to MGD. A full diagnosis was performed by means of clinical examination and in vivo confocal microscopy. C.STIM® intense pulsed light treatment plus eyelid care was initiated in this patient. After three months, a significant improvement in functional signs and meibum quality was observed, with almost no Demodex sleeves visible.
Anamnesis :
Mr J., aged 57, a teacher, consulted his doctor complaining of debilitating dry eye syndrome that had been present for several months. The prescribed symptomatic treatment had offered little relief. He was experiencing stinging, itching and photophobia. These symptoms mainly occurred in the morning, with fluctuating blurred vision upon blinking.